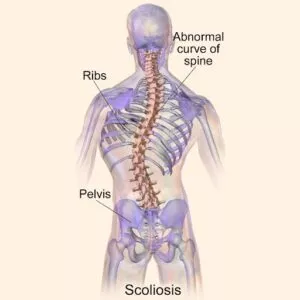
SCOLIOSIS
Scoliosis is a condition in which the spine curves abnormally from side to side, often taking on a “C” or “S” shape. It can affect people of all ages — from infants to older adults — and may cause pain, posture changes, and, in more severe cases, breathing or mobility issues.
According to the most comprehensive 2025 global meta-analysis involving over 42.9 million children and adolescents, the prevalence of scoliosis (confirmed by X-ray) is approximately 1.65% worldwide, with rates nearly twice as high in girls (1.76%) compared to boys (0.87%). In the United States, adolescent idiopathic scoliosis continues to affect an estimated 2–3% of teenagers, translating to roughly 6–9 million people. Prevalence tends to rise with age, and degenerative scoliosis becomes especially common in adults over 60, affecting up to 36–68% in some studies.
At the Southwest Scoliosis & Spine Institute, our board-certified, fellowship-trained spine surgeons have helped thousands of patients from Texas, Louisiana, Oklahoma, and beyond achieve better spinal health through early detection and personalized care.


3 percent of individuals with progressive curvature may eventually experience severe problems. This can include scoliosis and back pain, spinal problems, and nerve compression causing numbness, weakness, and leg pain.
Scoliosis & Pain
Deborah couldn’t remember a single day in her life without pain. That all changed when she had scoliosis surgery at Southwest Scoliosis and Spine Institute. Deborah had an 82-degree curve at the top of her spine and an 89-degree curve at the bottom. She was in terrible pain. She suffered from other spinal problems, including a scoliosis-caused chest deformity and it made it difficult to breathe. Even walking became difficult and she needed a cane to just walk 10 feet. “I was in so much pain, I felt like a zombie most of the time,” said Deborah. “I couldn’t work, shop or cook.”
At the Southwest Scoliosis and Spine Institute, We focus on Scoliosis Diagnosis, Treatment, & Care for our Patients
Our fellowship-trained, board-certified expert orthopedic scoliosis surgeons, Richard Hostin, MD, Devesh Ramnath, MD, Ishaq Syed, MD, Shyam Kishan, MD, and Kathryn Wiesman, MD specialize in all types of spine deformities and scoliosis pain. With our experience in research, diagnosis, treatment, and surgery for children, adolescents, and adults, the Southwest Scoliosis and Spine Institute is recognized as being at the top of the scoliosis specialty field. Our sought-after experienced doctors and surgical team are leaders in clinical outcomes for the spine conditions we treat. After years of providing great care and treatment, the Institute has received recognition for helping thousands of patients live pain-free. Also, our team treats and cares for patients with all types of spinal conditions, from mild cases to the most severe ones.
At the Southwest Scoliosis and Spine Institute, our team of spine specialists will devise the treatment plan for the patient. Furthermore, we will base the plan on the severity of the spinal curve. However, we also determine pain location and curve degree, the patient’s age, and the type of scoliosis. Our Doctors focus on the pain and correcting any deformity causing problems associated with the curve. Large numbers of patients live with pain and struggle with spine deformities that need our help. Because of our research and experience, we can often help with severe cases and help patients live pain-free enjoyable lives. Our unique perspective comes from actively conducting spine-specific research and treating very complex spine conditions. With this, we provide better surgical outcomes and patient satisfaction for both post-surgical treatment and scoliosis surgery.
Questions and Answers
Can a person live a normal life with Scoliosis?
Yes, many people with scoliosis can live normal lives. With appropriate treatment and management, including bracing, exercise, and regular check-ups, scoliosis patients can lead active and fulfilling lives. They can participate in activities they enjoy and maintaining an overall well-being.
How to live with Scoliosis
Living with scoliosis involves various strategies to manage the condition and maintain a good quality of life. This can include regular medical check-ups, following a prescribed treatment plan. In addition, practicing good posture, engaging in appropriate exercises and physical activities, and seeking support from doctors, family, and peers.
What are the treatment options for Scoliosis?
The treatment for scoliosis depends on several factors. These include the severity of the curvature, the age of the patient, and the underlying cause. Treatment options include observation for mild cases, bracing to prevent further progression in moderate cases, and surgery for severe cases. Our doctors may also recommend physical therapy and exercises to improve strength and flexibility in the spine.
We’re here to help STOP THE PAIN
Call 214-556-0555 or Email Us to make an appointment with our expert scoliosis and spine doctors.
Recognizing Scoliosis
Scoliosis refers to a side-to-side three-dimensional curvature of the spine. This curve can look like the shape of a “C” or a double curve, shaped like an “S”. Oftentimes, this condition gets diagnosed in childhood, occurring in both females and males. However, the condition mostly progresses in females, causing issues and pain later in life. This curve can cause deformity and all kinds of symptoms, including pain. The symptoms can exhibit minimal discomfort to really bad pain. Normally, as Scoliosis progresses, the pain gets worse, and body changes become more evident.
Epidemiology / Who Gets Scoliosis?
Doctors diagnose Scoliosis during the adolescent growth spurt (ages 10–18), but it can appear at any stage of life.
- Children & Adolescents: Idiopathic scoliosis accounts for the vast majority of cases. Mild curves (Cobb angle 10°–19°) make up about 87% of diagnosed cases, with the single thoracolumbar curve being the most common pattern. Prevalence has shown a slight upward trend since 2020.
- Adults & Older Patients: Many cases that began in adolescence continue into adulthood, while others develop later as degenerative scoliosis due to age-related wear on discs and joints. Rates climb significantly after age 50 and can reach 36–68% in people over 60.
Updated Screening & Early Detection
Risk factors include family history, female sex, poor posture, sedentary behavior, and limited outdoor time. Early school screenings in Texas (mandated for girls in 5th/7th grade and boys in 8th grade), along with programs in bordering states, Louisiana and Oklahoma, help catch many curves before they progress.
Learn more about scoliosis in specific age groups:
A positive screening result simply means a professional medical evaluation is recommended — most referred children have mild curves that respond well to monitoring or bracing. Early detection dramatically improves outcomes.
Related pages:
- What to Do If Your Child’s School Screening Suggests Scoliosis
- Scoliosis Screening in Schools
Understanding Scoliosis Classifications
Doctors categorize Scoliosis based on the degree of spinal curvature. These classifications help in determining the severity and appropriate treatment plans.
Types of Scoliosis Classifications:
Mild Scoliosis:
- Curvature: 25 degrees or less
- Characteristics: Often subtle and may not show prominent physical symptoms.
Moderate Scoliosis:
- Curvature: Between 25 and 40 degrees
- Characteristics: More noticeable and may require bracing to prevent further progression.
Severe Scoliosis:
- Curvature: Greater than 40 degrees
- Characteristics: Significant spinal deformity, potentially causing discomfort and requiring surgical intervention.
Understanding these classifications helps in early diagnosis and choosing the right treatment path, ensuring better management of scoliosis symptoms.
What Types of Scoliosis Can Certified Spine Doctors Treat?
Our certified doctors are equipped to handle a diverse range of scoliosis cases, catering to both moderate and severe conditions. They specialize in:
- Mild to Moderate Juvenile Scoliosis: Ideal for young patients where the curvature hasn’t shown rapid progression.
- Mild to Moderate Adolescent Scoliosis: Suitable for teenagers whose scoliosis is stable and doesn’t pose a high risk of worsening.
- Non-Surgical Adult Scoliosis: For adults with scoliosis cases that don’t necessitate surgical procedures, offering alternative treatment options to manage discomfort and curvature
- Progressive Scoliosis: For patients whose scoliosis is worsening over time, doctors can implement strategies to slow, halt, or even correct the curve progression.
- Severe Scoliosis: Cases with pronounced spinal curvature that might otherwise require surgical intervention can often benefit from the advanced treatment techniques our doctors use.
- Neuromuscular Scoliosis: Our certified doctors are trained to manage scoliosis resulting from neuromuscular disorders, providing specialized care for these complex conditions.
Our doctors have undergone rigorous training to speed up treatment processes while maintaining high standards of care, making them an excellent alternative to traditional bracing or less severe surgical interventions. Their expertise allows them to tailor intensive care regimens that effectively address the unique needs of each patient.
Diagnosing Scoliosis
First, your Scoliosis Doctor will examine your spine. The doctor will observe your spine while standing, bending, and walking. Then, if needed, your doctor will order and review your X-rays. Should your X-ray films reveal a curve in your spine, your doctor will measure it utilizing the Cobb Angle. This will let the doctor know if the curve in your spine appears mild, moderate, or severe.
Cobb angle
A Cobb angle is measured using X-ray imaging to calculate the degree to which the curve differs from normal alignment.
Cobb angle scale:
- 10-25 degrees – mild scoliosis
- 25-40 degrees – moderate scoliosis
- 40+ degrees – severe scoliosis
What Causes Scoliosis?
Although scientists and doctors study the causes of scoliosis, most of the time they do not know the answer. In fact, according to the Scoliosis Research Society (SRS), a specific cause is not found in 8 out of 10 cases. While many spine curvature cases are linked to genetics, there is no single cause that everyone can agree upon. Therefore, our current research is so important. In our research groups, we conduct research to enhance current conservative treatments by increasing their effectiveness. For example, we use state-of-the-art technology to improve post-surgery patient outcomes and more. All of this research helps our team develop new treatments and improve others.
Research also motivates us to learn to predict outcomes of different types of non-surgical treatments. We study how different surgery techniques affect patients after surgery and devise new surgical treatments for better patient outcomes. “To date, we have several findings, but there’s no unified theory of what causes Scoliosis curves,” says Dr. Hostin. “Thus, we don’t know why one person with a curve will progress to need a complex surgical procedure, while another with a curve that seems the same reaches adulthood and doesn’t need surgery.”
Several causations exist:
- Heredity – This curved spine condition tends to run in families with different effects in each generation, perhaps even skipping generations.
- Degenerative scoliosis can occur with age and osteoporosis.
- Spinal cord injury – A spine deformity can appear following a spinal cord injury or trauma. Also, spinal curvature patients who had polio in the 1930s, ’40s, and ’50s may have developed a spine curvature as a result of paralysis.
- Congenital – A spine curvature can result from the improper formation of vertebrae during fetal development.
- Neuromuscular – Abnormal nerve or muscle function can result in a large “C” shape in the spine.
Some of the conditions below may develop Scoliosis:
- Cerebral Palsy
- Spina Bifida
- Muscular Dystrophy
Doctors wonder if a scoliosis gene exists. Research is being conducted to identify specific genes that have a nexus with the curvatures of the spine. The hope is that doctors will someday predict which curves are at the highest risk for growth. “One cause of scoliosis might stem from genetics, and a result of many genes; however, it has variable penetrance, meaning that in each generation, genes act differently in how strongly they are expressed, which determines how severe a curve can progress,” explains Dr. Kishan. “This condition tends to run in families, but it tends to show different effects in each generation. For instance, a mother may have a mild curve and have a daughter with a severe curve. Or a mother with a severe curve may have grandchildren with a spine curvature, but the intervening generation had none.”
Common Forms of Scoliosis
- Congenital
- Degenerative
- Adolescent Idiopathic Scoliosis
- Lumbar
- Neuromuscular
- Thoracic
- Levoscoliosis
- Dextroscoliosis
- Pediatric Scoliosis (Scoliosis in Children)
- Early onset Scoliosis
What Are The Symptoms of Scoliosis?
A curved spine can exist as a hidden disorder with no obvious signs of curvature, or it can cause great discomfort, pain, and disability. Some patients have an undetected curvature of the spine for years until the curve starts to increase in size, causing pain and difficulty. “We think of scoliosis as being a childhood disease. However, most commonly, curvatures of the spine are diagnosed in the juvenile and adolescent stages. These are children aged 8, 9, 10, 11, and 12 years of age,” observes Dr. Hostin. “However, adult-onset or degenerative scoliosis, which we think develops as a result of disc degeneration, probably comprises an entirely separate entity from what we commonly think of as adolescent scoliosis.” Some symptoms include:
- A shoulder blade that appears higher than the other
- A pelvis that appears tilted
- Any imbalance in the rib cage or other deformities along the back
More Advanced Scoliosis Cases Exhibit:
- Back pain
- Neck pain
- Rib pain
- Difficulty breathing
- Headaches
- Limited movement
Scoliosis Pain
While most people with scoliosis do not get pain from the deformity it causes, some people may feel varying degrees of pain. The pain that sometimes comes with scoliosis is different from person to person, with the main factors involved being age and the severity of the condition.
Scoliosis will cause pain in the elderly with adult-onset scoliosis due to the pressure on spinal discs and facet joints, and the age-associated spinal degeneration that occurs. Also, the spinal curvature may cause contact with nerves, irritating them and inflaming joints. This can also cause mild or severe pain depending on the nerves and joints affected.
Scoliosis usually results in low back pain that requires urgent attention. Other painful symptoms include muscle tightening, painful sensations shooting down the legs, and uncomfortable postural changes. The aforementioned conditions can cause pain with movements over time.
What Are The Treatment Options For Scoliosis Based On Various Factors Such As Spinal Maturity, Degree Of Curvature, and Location Of The Curve?
When diagnosing scoliosis, the course of treatment is influenced by several critical factors. To start, it’s essential to consider the spinal maturity of the patient, determining whether the spine is still in its growth phase. The severity of the spinal curvature, along with its impact on the patient’s daily activities, is another crucial factor, as is the curve’s position along the spine, with thoracic spinal curves generally showing a higher tendency for worsening. Recognizing the potential for the curvature to increase, especially if it’s already substantial before the adolescent growth period, is also vital. Based on these assessments, medical professionals may recommend different approaches for managing scoliosis, including regular monitoring, the use of orthopedic braces, or surgical intervention to correct the curvature.
Scoliosis Treatment
Treatment depends on the patient’s age, curve severity (measured by Cobb angle), skeletal maturity, and symptoms. The goal is always to prevent progression while preserving function and quality of life.
Non-Surgical Options
For mild to moderate curves in growing children, bracing is the cornerstone of care. The landmark BrAIST study showed bracing prevents progression to surgical range in 72% of cases overall, rising to over 90% with 13+ hours of daily wear. Newer 2025–2026 data confirm that high-compliance bracing (18+ hours/day) achieves 97–98% success in keeping curves under 50° and 85–87% success in preventing meaningful progression. Modern 3D asymmetric braces (such as Rigo-Chêneau style) often provide even better correction than traditional designs.
Other non-surgical approaches include scoliosis-specific physical therapy, pain management (including heat therapy), and activity modification. Explore non-surgical care in depth
After variables are assessed, the doctor may suggest the following treatment:
Observation
In many children, a mild spinal curve does not require treatment. However, we recommend monitoring the child every four to six months through adolescence if there is a concern that the curve is becoming more severe. In adults with spine curvatures, X-rays are scheduled to track any progression or change.
Scoliosis identified in adults is distinct from that detected in children, primarily because the causes influencing the condition and the treatment strategies often vary after full skeletal development. In general, adults diagnosed with scoliosis fall into one of three groups: those who underwent surgical intervention for scoliosis during their adolescent years; those who were diagnosed during childhood but did not receive any treatment; and individuals diagnosed with degenerative scoliosis in adulthood, which typically arises due to wear and tear on the spine.
Bracing
After the evaluation, your doctor may want the patient to wear a brace. We brace patients who have not reached skeletal maturity. If the child continues to grow and his or her curve measures between 25 degrees and 40 degrees, the doctor may recommend a brace to prevent the curve from growing. As many different types of braces exist, your doctor will help you decide the best one for your child.
Braces are an effective treatment for scoliosis in patients who are still undergoing growth and have not yet reached skeletal maturity. They are typically recommended for children whose spinal curves are between 25 and 40 degrees to help prevent further curve progression. To achieve the best results, it is crucial that the brace fits properly and is worn diligently for 16 to 23 hours daily until the child stops growing. Various styles of braces are available, some newer designs offering under-arm fitting rather than around the neck, enhancing comfort without sacrificing efficacy. Recent large-scale studies have shown that with stringent adherence to the prescribed wearing schedule, braces effectively halt the progression of spinal curvature in approximately 80% of juvenile cases. Regular adjustments by a healthcare professional are necessary to ensure the brace continues to fit well as the child grows.
What Factors Do Doctors And Surgeons Consider When Weighing The Benefits And Risks Of Scoliosis Surgery?
When evaluating whether to proceed with scoliosis surgery, it’s crucial to balance potential gains against potential drawbacks. Success rates of surgical interventions can vary; while many individuals experience improvements, the surgery does not uniformly halt the progression of the spinal curvature or alleviate symptoms for all patients. Before making a decision, it’s advisable to consult with a neurosurgeon who can provide tailored medical advice and thoroughly discuss all treatment options.
Scoliosis Surgery
 In adults and children, the three primary goals of surgery are to stop the curve from progressing, to stop spinal deformity, and to stop the pain. Per our policy, we suggest surgery only when needed, and all other treatments have been tried. Our surgeons use spinal fusion, one of the most common procedures, to correct scoliosis. Surgical intervention is typically advised by medical professionals when the curvature of the spine exceeds 40 degrees and continues to worsen. Our surgeons adhere to guidelines established by leading bodies, such as the Scoliosis Research Society (SRS), an international organization specializing in spine care, and as such, we only use surgery when all other treatments fail.
In adults and children, the three primary goals of surgery are to stop the curve from progressing, to stop spinal deformity, and to stop the pain. Per our policy, we suggest surgery only when needed, and all other treatments have been tried. Our surgeons use spinal fusion, one of the most common procedures, to correct scoliosis. Surgical intervention is typically advised by medical professionals when the curvature of the spine exceeds 40 degrees and continues to worsen. Our surgeons adhere to guidelines established by leading bodies, such as the Scoliosis Research Society (SRS), an international organization specializing in spine care, and as such, we only use surgery when all other treatments fail.
Minimally invasive surgery (MIS) for scoliosis treatment involves performing surgical procedures with smaller incisions compared to traditional surgery. This approach utilizes sophisticated tools such as fluoroscopy and endoscopy, which aid in precision. Fluoroscopy provides real-time X-ray imaging during the operation, allowing precise placement of surgical hardware, while endoscopic techniques employ a camera to give surgeons a clear view of the operation area. The key benefits of this technique include reduced tissue damage and less post-operative pain, leading to quicker recovery times. However, it’s important to note that MIS is not suitable for all scoliosis cases; the choice of surgical technique is influenced by various factors specific to each patient.
Understanding Minimally Invasive Surgery (MIS)
Minimally invasive surgery (MIS) for scoliosis involves performing procedures through small incisions rather than the large ones required in traditional surgery. This technique utilizes state-of-the-art technologies such as fluoroscopy and endoscopy. Fluoroscopy provides real-time X-ray images of the back, assisting surgeons in navigating during the procedure. Endoscopy involves the use of a camera, inserted through the incision, that gives a detailed view of the spine. Both technologies improve the precision of surgical movements and the placement of surgical hardware.
When should surgeons use MIS for Scoliosis?
MIS isn’t suitable for every scoliosis patient. Its viability depends on several factors, including the severity and location of the curve, the patient’s overall health, and their medical history. The following provides key details:
- Severity and Type of Curve: Not all spinal curves are amenable to MIS techniques. Generally, less severe and less complex curves are better candidates.
- Body Size: Patients with certain body sizes might benefit more from traditional surgery.
- Previous Surgeries: Previous spinal surgeries might affect the feasibility of using MIS methods.
In addition to these factors, the choice of surgical method, including whether to opt for MIS, also hinges on the technological advancements utilized during the procedure. Minimally invasive surgery often employs advanced fluoroscopy and endoscopy. These technologies help minimize tissue trauma and enhance the accuracy of incisions and hardware placement. Such precision is crucial, particularly when the surgical site is accessed through smaller incisions, which characterizes MIS.
However, surgeons understand that MIS cannot treat all cases. The decision to employ this technique is influenced not only by patient-specific factors but also by the overall goals of the surgery, such as achieving better deformity correction or quicker patient rehabilitation. These objectives might sometimes necessitate more traditional approaches, especially when dealing with more complex spinal deformities or when previous surgeries complicate the anatomical landscape.
By considering both the patient-specific factors and the technical capabilities of MIS, healthcare providers can make informed decisions that optimize treatment outcomes for scoliosis patients.
Decompressive laminectomy: and when should surgeons recommend it for scoliosis and spinal stenosis?
A decompressive laminectomy is a surgical procedure designed to alleviate pressure on the spinal nerves by widening the spinal canal. When individuals have conditions such as scoliosis—a curvature of the spine—and spinal stenosis, which involves the narrowing of the spinal canal, this procedure is commonly recommended. To maintain spinal stability, especially in cases involving these conditions, the surgery may also incorporate spinal fusion and possibly the addition of spinal instrumentation to ensure the spine remains stable after the procedure.
The Surgical Procedure Explained:
In a decompressive laminectomy, surgeons remove the laminae, which are the back parts of the vertebrae forming the roof over the spinal canal. Removing these structures provides additional space for the nerves, thus relieving pressure and pain.
When is it recommended?
This procedure is particularly recommended for scoliosis patients who:
- Experience significant spinal nerve compression due to spinal stenosis
- Continue to suffer from persistent pain or neurological symptoms despite other treatments
- Have noticeable instability in the spine sections affected by scoliosis and stenosis
Decompressive laminectomy offers a viable solution for those affected by the simultaneous occurrence of scoliosis and spinal stenosis, aiming to improve both spinal function and quality of life.
The anterior approach for scoliosis surgery and its potential advantages and disadvantages
The anterior approach for scoliosis surgery involves the patient being positioned on their side. During the procedure, the surgeon accesses the spine through incisions made on the side of the patient’s body. To facilitate a clear path to the spine, one lung is temporarily deflated, and a rib is removed if necessary. This method can also utilize video-assisted thoracoscopic (VAT) surgery, which not only improves the surgeon’s view of the spinal area but is considered less invasive compared to traditional open surgery.
Advantages of the Anterior Approach
There are several potential advantages to using the anterior approach in scoliosis surgery:
- Effective Correction of Deformities: This approach allows for better correction of spinal deformities.
- Faster Patient Rehabilitation: Patients tend to recover more quickly, facilitating faster return to daily activities.
- Improved Spine Mobilization: Surgeons can enhance the spine’s mobility by a precise correction and alignment.
- Fewer Segments Fused: Typically, this approach requires the fusion of fewer spinal segments, preserving more of the spine’s natural movement.
Potential Disadvantages
However, the anterior approach is not without its challenges:
- Post-Surgical Bracing: Patients often need to wear a brace for several months following the procedure to support the spine as it heals.
- Higher Risk of Complications: While the use of VAT has mitigated some risks, the approach still carries a higher risk of complications compared to other surgical methods.
By utilizing the anterior spinal approach, the surgeon can achieve a more accurate and less invasive correction of spinal deformities, though it requires careful consideration of the potential risks and postoperative care.
Posterior spinal fusion with instrumentation and bone grafting surgery for scoliosis
The posterior spinal fusion with instrumentation and bone grafting surgery is a common procedure for treating adolescent idiopathic scoliosis. It is conducted with the patient face down. The main steps include the insertion of rigid rods to correct the alignment of the spine, making it straighter. Following this, the surgeon performs a spinal fusion, which entails placing bone graft material along the areas of curvature. This helps in forming a bony bridge that fuses segments of the spine, thereby stabilizing the correction achieved by the rods. These metal rods are crucial as they support the spine in its new alignment while the fusion solidifies.
The differences between the posterior and anterior surgical approaches for scoliosis treatment
The surgical approaches to treating adolescent idiopathic scoliosis vary primarily in terms of the incision placement and the overall surgical process, each with its distinct advantages and possible complications. In the posterior approach, surgeons perform the procedure with the patient prone (lying facedown). This technique involves the insertion of metal rods to stabilize and straighten the spine, which is followed by a spinal fusion. The fusion process includes placing a bone graft along the affected parts of the spine to facilitate the fusion of the vertebrae, ensuring the spine remains straight after surgery.
Conversely, the anterior approach requires the patient to lie on the side. Surgeons access the spine through side incisions, which may involve temporarily deflating a lung and removing a rib to better reach the spinal area. This method often utilizes video-assisted thoracoscopic surgery (VATS), which enhances the view of the operative field while being less intrusive compared to traditional open surgery. The benefits of the anterior approach include potentially more precise correction of the deformity and faster recovery times. This method can also result in more effective spinal mobilization and might require the fusion of fewer spinal segments compared to the posterior approach.
However, it often necessitates postoperative bracing and carries a greater risk of complications, though the use of VAT techniques mitigates some of these risks. Each approach, therefore, maintains distinct procedural differences and considerations, influencing the choice of technique based on specific patient needs and the nature of the scoliotic curvature.
What Factors Can Lead to Increased Surgical-Related Risks In Older Adults With Degenerative Scoliosis?
Older adults with degenerative scoliosis facing surgery may encounter heightened risks due to several factors: their advanced age, a history of smoking, excess body weight, and existing health or medical issues. Some adults who were treated as children may need revision surgery. For instance, if treatment occurred 20 to 30 years ago, before major advances in spinal surgery were implemented.
Oftentimes, the adult patient will get new symptoms, mainly severe back pain, trouble walking, or broken hardware. Another reason for revision surgery occurs when the lordosis does not function correctly, like flatback syndrome. In general, the doctor may recommend surgery when science reveals that surgery will improve the quality of life.
When Do Doctors Typically Recommend Surgery For Adults With Scoliosis?
Surgery is typically recommended for adults with scoliosis when their spinal curvature exceeds 50 degrees, and they exhibit symptoms like nerve damage affecting their legs or problems with bowel or bladder control. Additionally, adults who have degenerative scoliosis accompanied by spinal stenosis might need to undergo decompression surgery paired with spinal fusion, involving surgical procedures from both the anterior and posterior sides.
The primary goals of surgery for children with scoliosis
The main objectives of performing surgical procedures on children with scoliosis are to prevent further curvature of the spine as they mature into adulthood and to reduce the existing spinal deformity. Surgical intervention is typically advised by medical professionals when the curvature of the spine exceeds 40 degrees and continues to worsen.
Scoliosis Statistics:
Prevalence:
- 2-3% of the population: This translates to roughly 6-9 million people in the United States alone.
- Equal prevalence between genders: However, females are 8 times more likely to require treatment due to curve progression.
Age of Onset:
- Primary age: 10-15 years old: For this age, doctors use the term adolescent idiopathic scoliosis (AIS), which appears as the most common type.
- Can develop earlier or later: Scoliosis can also occur in infancy, childhood, and adulthood.
Treatment:
- Only a small percentage (30%) require bracing: Monitoring provides sufficient care for mild curves.
- Even fewer (10%) require surgery: This provides solutions for severe curves that impact health or aesthetics.
- Yearly visits to doctors: Over 600,000 occur for scoliosis concerns.
- 30,000 children fitted with braces: This helps manage curve progression during growth.
- 38,000 patients undergo spinal fusion: This surgery aims to permanently correct the spinal curvature.
Additional Statistics:
- Pain: 63% of children with scoliosis report pain, compared to 31% without.
- Pain severity: 23% of scoliosis patients rate their pain as “horrible,” exceeding those without scoliosis.
- Emergency room visits: Over 90,000 annually, highlighting potential complications.
- Adult considerations: 40% of adults with scoliosis experience curve progression, though usually mild.
Living with Scoliosis
With today’s screening programs, advanced bracing, and refined surgical techniques, the vast majority of people with scoliosis lead active, healthy lives. Early intervention, whether through school screening or prompt specialist evaluation, is the key to the best outcomes.
At the Southwest Scoliosis & Spine Institute, our team provides world-class, compassionate care for patients of all ages at our convenient locations in Dallas, Plano, and Frisco. Families from Texas, Louisiana, Oklahoma, and across the Southwest regularly travel to us for expert scoliosis evaluation, custom bracing, and advanced treatment.
Schedule a consultation today and take the first step toward a straighter, more comfortable future.
Why Choose the Southwest Scoliosis and Spine Institute
Unfortunately, many cities do not have doctors who specialize in Scoliosis. Therefore, many patients must travel to other cities to obtain the benefits from Scoliosis Specialists to improve their lives. Only a handful of surgeons have extensive experience and training to specialize in these difficult, life-changing procedures. Thus, patients come to us from around the world to restore a pain-free life. While many patients with spinal curves believe that treatment does not exist, our practice offers medical solutions. Our solutions are based on proven medical techniques and facts.
From the first time you walk into our Southwest Scoliosis and Spine Institute offices in either Dallas, Plano, or Frisco, Texas, you will feel at ease. You will talk to one of our expert doctors. Our doctors will listen to and understand your problem, and then perform a detailed examination. The doctor will review your X-rays and other tests with you in detail and provide a diagnosis. After you become well-informed, you and your doctor will plan the right treatment. Finally, if your scoliosis doctor or spine surgeon feels that surgery will not provide the desired result, he’ll tell you that too, and offer a non-surgical remedy as the first course of treatment.
Expertise and Excellence
Our expert spine specialists have received many academic honors & awards and have published articles in several peer-reviewed journals. Additionally, they have presented their work at national and international meetings. In addition, they are also members of several noted research societies, including the American Academy of Orthopaedic Surgeons, Pediatric Orthopaedic Society of North America, Scoliosis Research Society, American Orthopaedic Association, and the Growing Spine Study Group. We invite you to schedule an appointment at one of our Scoliosis Centers, and usually, we can get you in within 24 hours.
_____________________________________
Citation: Scoliosis Research Society – Scoliosis Information and Support
The medical content on this page has been carefully reviewed and approved for accuracy by the Southwest Scoliosis and Spine Institute’s qualified healthcare professionals, including our board-certified physicians and Physician Assistants. Our team ensures that all information reflects the latest evidence-based practices and meets rigorous standards of medical accuracy, with oversight from our expert spine doctors to guarantee reliability for our patients.
Definitions:
The atlas refers to the first cervical vertebra and its location appears between the skull and the rest of the spine. Additionally, the atlas does not have a vertebral body, but it does have a thick forward (anterior) arch and a thin back (posterior) arch with two prominent sideways masses.
In addition, the atlas sits on top of the second cervical vertebra, the axis. The axis has a bony knob called the odontoid process, which sticks up through the hole in the atlas. Special ligaments between the atlas and the axis allow for a great deal of rotation. Also, this unique situation allows the head to turn from side to side as far as it can.
The cervical spine is very flexible, but it is also very much at risk for injury from strong, sudden movements, such as whiplash-type injuries. This high risk of harm occurs due to the limited muscle support that exists in the cervical area, and the fact that this part of the spine supports the weight of the head, which weighs an average of 15 pounds. This is a lot of weight for a small, thin set of bones and soft tissues to bear. Accordingly, sudden, strong head movements can cause damage.
If you are an adult living with scoliosis or have a child with scoliosis and need a doctor who specializes in orthopedic surgery,
call the Southwest Scoliosis and Spine Institute at 214-556-0555 to make an appointment today.